Overview of Sever’s Disease
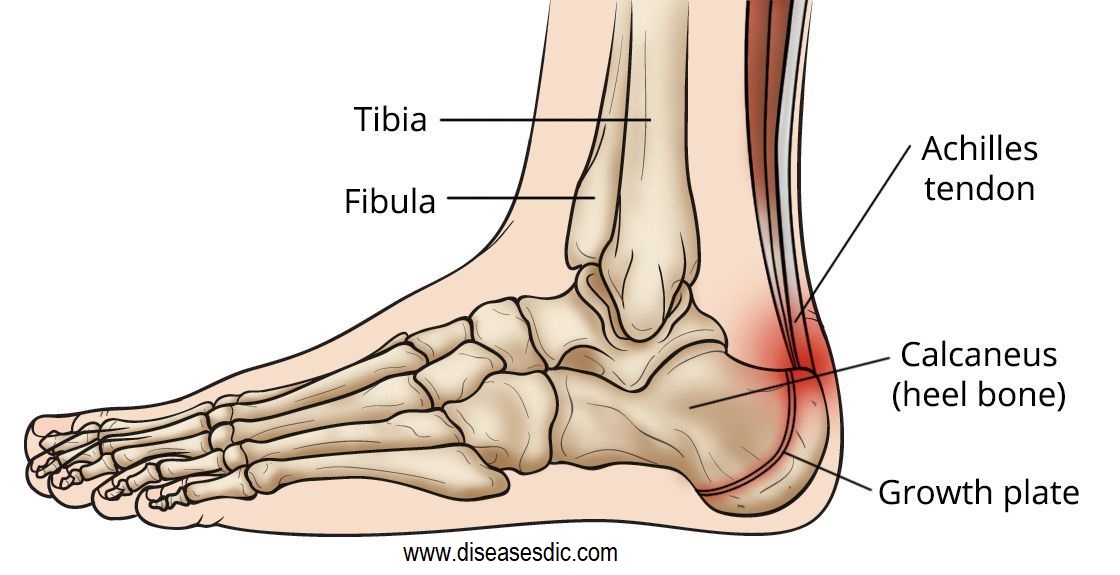
Sever’s disease or Calcaneal Apophysitis is a painful condition of the heel that occurs in growing children. It happens when the tendon that attaches to the back of the heel (the Achilles tendon) pulls on the growth plate (the apophysis) of the bone of the heel (the calcaneus). The repeated stress on the growth plate causes pain and inflammation at that site.
It most commonly occurs in physically active children between the ages of 8 and 14 years of age. This pain is often worsened by physical activity or when Achilles tendons are tight. Pain can also be worse during a “growth spurt,” when the bones grow faster than the tendons. This increases the pull of the tendon on the heel. While painful, Sever’s disease is not a serious condition. It will not cause long term damage or arthritis and often resolves once the growth plates close.
Pathophysiology of Sever’s Disease
The calcaneal apophysis develops as an independent center of ossification (possibly multiple). It appears in boys aged 9-10 years and fuses by age 17 years; it appears in girls at slightly younger ages. During the rapid growth surrounding puberty, the apophyseal line appears to be weakened further because of increased fragile calcified cartilage.
Microfractures are believed to occur because of shear stress leading to the normal progression of fracture healing. This theory explains the clinical picture and the radiographic appearance of resorption, fragmentation, and increased sclerosis leading to eventual union. The radiographs showing fragmentation of the apophysis are not diagnostic, because multiple centers of ossification may exist in the normal apophysis, as noted. However, the degree of involvement in children displaying the clinical symptoms of Sever disease appears to be more pronounced.
Causes of Sever’s Disease
Overuse and stress on the heel bone through participation in sports is a major cause of calcaneal apophysitis. The heel’s growth plate is sensitive to repeated running and pounding on hard surfaces, resulting in muscle strain and inflamed tissue. For this reason, children and adolescents involved in soccer, track, or basketball are especially vulnerable.
Other potential causes of calcaneal apophysitis include obesity, a tight Achilles tendon, and biomechanical problems such as flatfoot or a high-arched foot.
Risk factors that contribute to sever’s disease
Sever’s disease is age- and activity-related. It usually starts in pre-teens and maybe more common in pre-teens who are physically active. It occurs when the calcaneal (heel) apophysis is open and active.
Factors that may contribute to Sever’s disease in pre-teens include changes in:
- Height and weight
- How much physical activity they are doing – this may be an increase in volume, intensity or frequency of activity. This commonly occurs:
- As one sports season ends and another starts
- Where there is crossover in sport
- When a child starts to train and play for a team (the volume of activity increases with multiple weekly training sessions and a game)
- When they are involved in a sports carnival which involves playing multiple games in one day or over a number of days
- Frequency of physical activity
- The type of physical activity – such as starting a different activity, or returning to physical activity after a break. Sever’s disease is most commonly associated with sports and activities that are weight-bearing, such as sports that involve running or jumping or both (for example, football, netball, running and gymnastics)
- Equipment or external factors – such as changing to shoes with a low heel (for example, football boots or some types of running shoes; the lower heel adds extra load to the apophysis, because it places the Achilles tendon on increased stretch), doing a sport in bare feet, or even walking at the beach in thongs/flip flops.
Physical attributes that may contribute to developing Sever’s disease include:
- Foot posture – active children who have a flat foot posture may be slightly more predisposed to Sever’s disease
- Increased body weight, or
- A high BMI (body mass index).
Characteristics/Clinical Presentation of Sever’s Disease
This disease can occur unilaterally or bilaterally. The incidence of bilaterally is approximately 60%. Common signs and symptoms:
- Posterior inferior heel pain (over the medial and lateral surface of the bone)
- Pain is usually absent when the child gets up in the morning
- Increased pain with weight-bearing, running or jumping (= activity-related pain)
- The area often feels stiff
- The child may limp at the end of physical activity
- Tenderness at the insertion of the tendons (avascular necrosis of the arthropathy)
- Limited ankle dorsiflexion range secondary to tightness of the Achilles tendon
- Hard surfaces and poor-quality or worn-out athletic shoes contribute to increased symptoms
- The pain gradually resolves with rest
What are the complications of Sever’s disease?
There are no serious complications associated with the condition. Although Sever’s disease can come and go as your child is growing, it does not cause long-term health problems. Children grow out of the condition as they age and their growth plates harden into solid bone.
How is Sever’s disease diagnosed?
Sever’s disease is based on the symptoms reported. To confirm the diagnosis, the clinician will examine the heels and ask about the child’s activity level and participation in sports. They may also squeeze the back part of the heel from both sides at the same time to see if doing so causes pain and also ask the child to stand on tiptoes to see if that position causes pain. There may be tightness in the calf muscle, which contributes to tension on the heel. Symptoms are usually worse during or after activity and get better with rest. X-rays generally are not that helpful in diagnosing Sever’s disease, but they may be ordered to rule out other problems, such as fractures. Sever’s disease cannot be seen on an X-ray.
How sever’s disease is It Treated?
Sever’s disease treatment should be based on eliminating pain and restoring normal foot and leg biomechanics.
Phase 1 – Early Injury Protection: Pain Relief & Anti-inflammatory Tips
As with most soft tissue injuries the initial treatment is Rest, Ice, and Protect.
In the early phase you’ll most likely be unable to walk pain-free. Our first aim is to provide you with some active rest from pain-provoking activities.
“No Pain. No Gain.” does not apply in Sever’s disease. If it hurts your child is doing too much exercise. Your child should reduce or cease any activity that causes heel pain.
Ice is a simple and effective modality to reduce your pain and swelling. Please apply for 20-30 minutes each 2 to 4 hours during the initial phase or when you notice that your injury is warm or hot.
Most children can tolerate paracetamol as pain-reducing medication. Check with your doctor.
To support and protect your heels, you may need to be wear shock absorbing heel cups or a soft orthotic. Kinesio foot taping may help to provide pain relief.
Your physiotherapist will guide you and utilize a range of pain-relieving techniques including joint mobilizations for stiff ankle or subtalar joints, massage or electrotherapy to assist you during this pain-full phase.
Phase 2: Regain Full Range of Motion
Your physiotherapist will identify stiff joints within your foot and ankle complex that they will need to loosen to help you avoid overstress. A sign that you may have a stiff ankle joint can be a limited range of ankle bend during a squat maneuver. Your physiotherapist will guide you.
Phase 3: Restore Foot Arch Muscle Control
Your foot arch is dynamically controlled via important foot arch muscles, which be weak or have poor endurance. These foot muscles have a vital role as the main dynamically stable base for your foot and prevent excessive loading through your plantar fascia.
Any deficiencies will be an important component of your rehabilitation. Your physiotherapist is an expert in the assessment and correction of your dynamic foot control. They will be able to help you to correct your normal foot biomechanics and provide you with foot stabilization exercises if necessary.
Phase 4: Restore Normal Calf & Leg Muscle Control
You may find it difficult to comprehend, but all of your leg (calf, thigh, and hip) muscles play an important role in controlling your foot arch and its normal function. are very important in the rehabilitation of shoulder pain and injury. Your physiotherapist will assess your leg muscle function and provide you with the necessary treatment or exercises as required.
Phase 5: Restore Normal Foot Biomechanics
Your foot biomechanics are the main predisposing factor to Sever’s disease. After a biomechanical assessment you may be recommended a soft orthotic or a custom made orthotic prescribed by a podiatrist.
Phase 6: Improve Your Running and Landing Technique
In order to prevent a recurrence as you return to sport, your physiotherapist will guide you with technique correction and exercises to address these important components of rehabilitation to both prevent a recurrence and improve your sporting performance.
Your physiotherapist will discuss your goals, time frames and training schedules with you to optimize you for a complete return to sport.
Phase 7: Footwear Analysis
Poorly designed footwear that can predispose to the injury. Seek the professional advice of your healthcare practitioner
What about Orthotics or Heel Cups?
Occasionally, an orthotic may need to be prescribed for temporary or long-term correction of their foot biomechanics (eg flat feet or high arches).
During the acute phase of Sever’s disease, a small heel rise or shock-absorbing heel cup placed under the heel pad of your child’s foot may help to ease the symptoms.
Your podiatrist or physiotherapist can assess your child’s arch and guide you in the best management of your child’s condition. We recommend that your child should never go barefooted during the painful stages of Sever’s disease.
How can you prevent Sever’s disease?
It may not be possible to prevent Sever’s disease, especially in very active children. To reduce the risk of your child developing the condition, you can:
- Maintain a healthy weight: Children who are overweight or obese are more likely to have Sever’s disease. Encourage your child to eat healthy foods and stay active to keep their weight in the normal range.
- Encourage rest: Tell your child to take a break from activities if pain or swelling occurs. Children who give their bodies time to heal between activities have a lower risk of developing Sever’s disease.
- Choose the right shoes: Children should wear supportive footwear that is appropriate for the sport or activity. Cleats can make symptoms worse because they put more pressure on the heel.
- Vary the activities: If your child participates in a lot of high-impact sports that involve running and jumping, mix in some low-impact activities. Swimming and bike riding will keep your child active while reducing stress on the heel bone.





My feet eat a lot and burn and blood comes out of it, it hurts when walking
Please consult a doctor to get treated with this problem.