



Overview
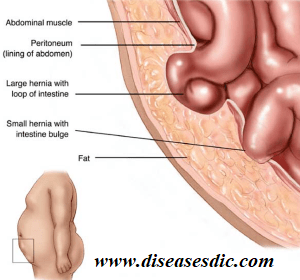
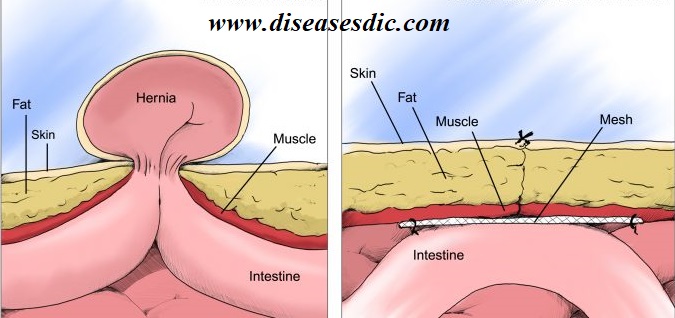
A hernia occurs when an organ pushes through an opening in the muscle or tissue that holds it in place. For example, the intestines may break through a weakened area in the abdominal wall. Hernias are most common in the abdomen, but they can also appear in the upper thigh, belly button, and groin areas. Most hernias aren’t immediately life-threatening, but they don’t go away on their own. Sometimes they can require surgery to prevent potentially dangerous complications.


Types of Hernia
There are many types of hernias. The most common types of hernia include:
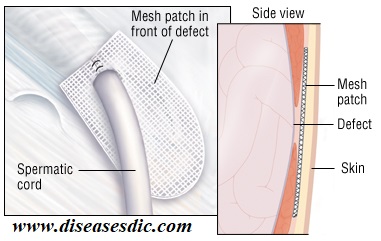
- Inguinal hernia (inner groin): This is the most common type of hernia, especially among men, and occurs when the intestines push through a weak spot or tear in the lower abdominal wall, often in the inguinal canal. This type of hernia is associated with aging and occurs if the abdomen is repeatedly strained. In men, the inguinal canal area is where the spermatic cord passes from the abdomen to the scrotum. This cord holds up the testicles. In women, the inguinal canal contains a ligament that holds the uterus in position.
- Incisional hernia (resulting from an incision): This condition may occur to some people who have undergone abdominal surgery. The intestines may push through the incision scar or the surrounding, weak tissue.

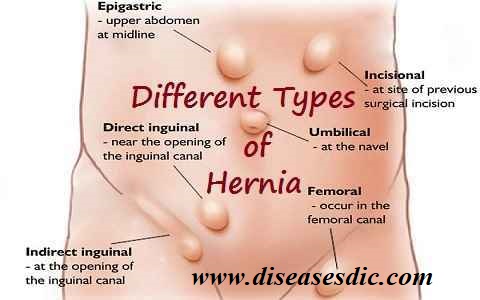
- Femoral hernia (outer groin), umbilical (belly button): This condition tends to occur more in women than men. It occurs when fatty tissue or a part of your bowel spill through into your groin at the top of your inner thigh. Like inguinal hernia, this type of hernia is associated with ageing and occurs due to repeated strain on the abdomen.
- Hiatal hernia (upper stomach): This condition is most common in people over 50 years of age and occurs when part of the stomach protrudes up through the diaphragm into the chest cavity. Hiatal hernias can cause gastroesophageal reflux, which is when the stomach contents leak back into the esophagus, causing a burning sensation in the heart.
- Umbilical hernia: This type of hernia occurs when fatty tissue or a part of the bowel pokes through the abdomen near the belly button.
Causes of Hernia
Hernias are caused by a combination of muscle weakness and strain. Depending on its cause, a hernia can develop quickly or over a long period of time.
Common causes of muscle weakness include:
- Failure of the abdominal wall to close properly in the womb, which is a congenital defect
- Age
- Chronic coughing
- Damage from injury or surgery
Factors that strain your body and may cause a hernia, especially if your muscles are weak, include:
- Being pregnant, which puts pressure on your abdomen
- Being constipated, which causes you to strain when having a bowel movement
- Lifting heavyweight
- Fluid in the abdomen, or ascites
- Suddenly gaining weight
- Surgery in the area
- Persistent coughing or sneezing
Risk factors of Hernia
The risk factors can be broken down by hernia type:
Incisional hernia risk factors
Because an incisional hernia is the result of surgery, the clearest risk factor is a recent surgical procedure on the abdomen.
People are most susceptible 3-6 months after the procedure, especially if:
- They are involved in strenuous activity
- Have gained additional weight
- Become pregnant
These factors all put extra stress on tissue as it heals.
Inguinal hernia risk factors
Those with a higher risk of inguinal hernia include:
- Man smoking a cigarette in a darkened room
- Older adults
- People with close relatives who have had inguinal hernias
- People who have had inguinal hernias previously
- Males
- Smokers, as chemicals in tobacco, weaken tissues, making a hernia more likely
- People with chronic constipation
- Premature birth and low birth weight
- Pregnancy
Umbilical hernia risk factors
Umbilical hernias are most common in babies with low birth weight and premature babies.
In adults, the risk factors include:
- Being overweight
- Having multiple pregnancies
- Being female
Hiatal hernia risk factors
The risk of hiatal hernia is higher in people who:
- Are aged 50 years or over
- Have obesity
Signs and Symptoms
External Hernia Symptoms
The most common hernias are external, although this category covers a few different types of hernia.
- Inguinal hernias are the most common type of hernia. They happen when a section of intestine or fatty tissue pushes through the abdominal wall in the groin area, at the top of your inner thigh.
- Femoral hernias also affect the groin but involve a different area of muscle weakness. They’re much less common than inguinal hernias.
- Umbilical hernias involve a section of intestine or fatty tissue pushing through the abdominal wall near the navel (belly button).
- Incisional hernias happen in an area where an incision was made for prior abdominal surgery. Fatty tissue or part of your intestine can push through your abdominal wall at the incision site.

The location of each of these hernia types vary, and not all of them will cause the same symptoms. But the most common symptoms of an external hernia include the following:
- A noticeable lump or bulge in the groin or abdomen
- A bulge that can be pushed back in or disappears when lying down
- An increase in the size of the bulge over time
- Swelling, pain, or a bulge in the groin or scrotum in men
- Pain or a burning or aching sensation at the site of the bulge
- Pain while coughing, bending over, or lifting heavy objects
- A heavy feeling in your groin
- Weakness or a feeling of pressure in your groin
- A sense of fullness or bowel obstruction
Internal Hernia Symptoms
Unlike an external hernia, an internal hernia will not create a bulge on the outside of your body.
One of the most common types of internal hernia is a hiatal hernia, in which part of the stomach pushes up through the diaphragm, the sheet of muscle that separates your abdomen from your chest.
In many cases, a hiatal hernia doesn’t cause any symptoms.
But sometimes a hiatal hernia can cause digestive juices in the stomach to move up into the esophagus, known as acid reflux, or gastroesophageal reflux disorder (GERD).
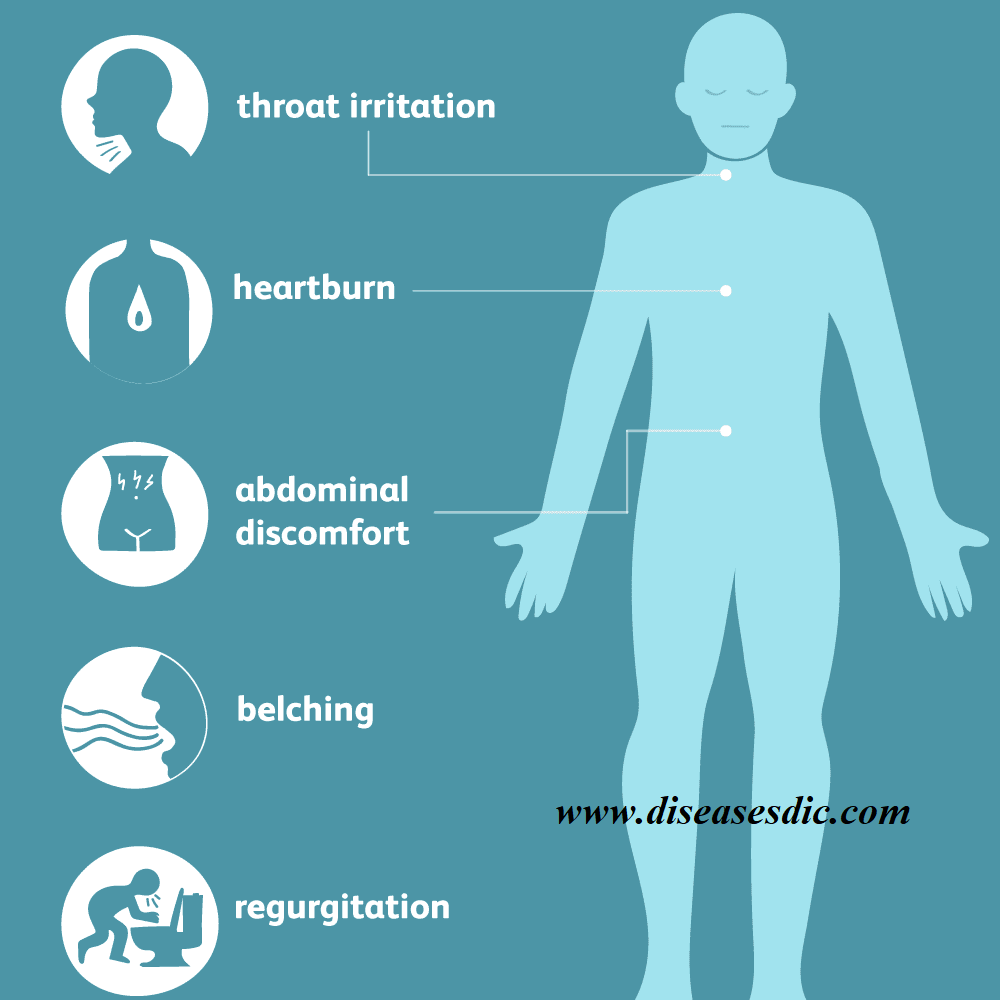
Symptoms of GERD include these reactions:
- Heartburn (a burning sensation in the upper chest)
- An acidic, bitter, or sour taste in the back of your throat
- A bloated feeling in your stomach
- Frequent belching (burping)
- Discomfort or pain in your stomach or esophagus
Hiatal hernias don’t always cause GERD, and most cases of GERD aren’t caused by a hiatal hernia, so these symptoms, or a lack of them, can’t definitively let you know whether you have this condition.
A hiatal hernia can also cause chest pain, which may be a symptom of a heart attack. If you experience chest pain, it’s important to call or see a doctor right away.
There are several other relatively rare types of internal hernias, most of which involve areas of the digestive tract pushing through surrounding structures and tissues.
These hernias are often the result of abdominal surgery, especially certain kinds of gastric bypass operations. But they can also be the result of congenital (present since birth) openings or weaknesses in internal abdominal structures, the most common of which is known as a paraduodenal hernia.
Complications
Other than umbilical hernias in babies, hernias will not disappear on their own. Over time, a hernia can grow larger and more painful or can develop complications.
Complications of an untreated inguinal or femoral hernia may include:
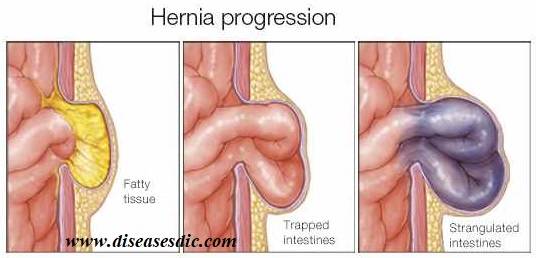
- Obstruction (incarceration): Part of the intestine becomes stuck in the inguinal canal, causing nausea, vomiting, stomach pain, and a painful lump in the groin.
- Strangulation: Part of the intestine is trapped in a way that cuts off its blood supply. In such cases, emergency surgery (within hours of occurring) is necessary to prevent tissue death.
Diagnosis and Test
Hiatus hernia is most commonly diagnosed when doctors do an endoscopy to investigate reflux, or when a barium X-ray has been performed. The hiatus hernia can show up as a bulge that is positioned between the oesophagus and your stomach. Large hiatus hernias can be observed on plain chest X-rays.
Herniagram
This is a special x-ray (not often done now, partly because it is ‘invasive’) that involves an injection with a needle. A liquid that shows on x-rays (radio-opaque) has to be injected into the abdominal cavity. If there is a hernia (hole in the abdominal wall) the liquid trickles through the hole and can be seen on the x-ray. It’s sometimes helpful if there is a question about whether a previously repaired hernia has returned
Barium X-ray
A barium swallow test or barium meal is a test in which you will be asked to drink a chalky liquid containing barium that helps your internal organs show up more clearly on X-ray pictures. The barium will outline your gullet, stomach and upper part of your small intestine. This test may help your doctor see whether you have a hiatus hernia.
Endoscopy or gastroscopy
Another way your doctor may check for a hiatus hernia is by referring you for a gastroscopy, which is an endoscopic examination. This is where you are given a light sedative and a doctor will insert a thin flexible lighted tube (an endoscope) down into your esophagus (gullet).

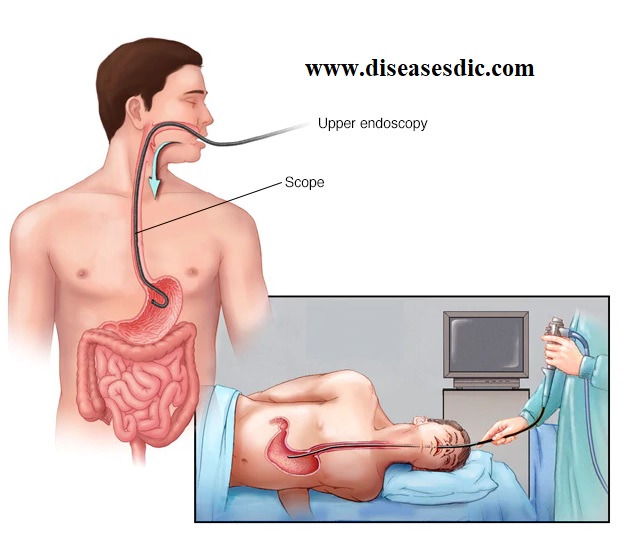
The tube allows the doctor to ‘look’ at your esophagus and check for abnormalities. This common procedure is usually painless and is generally performed in day surgery centers in public or private hospitals.
Ultrasound
Similar to the ultrasound exam used for pregnant women. Ultrasound gives a shadowy black and white picture. The result is operator dependent, meaning it depends on who is doing it.
Treatment and Medication
Hernias usually do not get better on their own, and surgery may be the only way to repair them. However, your doctor will recommend the best therapy to address your hernia and may refer you to a surgeon. If the surgeon thinks it is necessary to repair your hernia, then the surgeon will tailor the method of repair that best meets your needs.
In the case of an umbilical hernia in a child, surgery may be recommended if the hernia is large or if it has not healed by the age of 4–5 years old. By this age, a child can usually avoid surgical complications.
If an adult has an umbilical hernia, surgery is usually recommended because the condition will not likely improve on its own and the risk of complications is higher.
One of three types of hernia surgery can be performed:
Open surgery, in which a cut is made into the body at the location of the hernia. The protruding tissue is set back in place and the weakened muscle wall is stitched back together. Sometimes a type of mesh is implanted in the area to provide extra support.

Laparoscopic surgery involves the same type of repairs. However, instead of a cut to the outside of the abdomen or groin, tiny incisions are made to allow for the insertion of surgical tools to complete the procedure.

Robotic hernia repair, like laparoscopic surgery, uses a laparoscope and is performed with small incisions. With robotic surgery, the surgeon is seated at a console in the operating room and handles the surgical instruments from the console. While robotic surgery can be used for some smaller hernias or weak areas, it can now also be used to reconstruct the abdominal wall.
Postoperative Care after Hernia Repair
After hernia repair surgery, the patient is taken to the postanesthesia care unit (PACU). Patients are closely monitored by the nursing staff and remain there until they are stable. The amount of time spent in the PACU depends on the patient’s progress and on the type of anesthesia they received. Patients given general anesthesia must be awake and coherent before they leave the PACU.
Ice chips are offered to the patient in the PACU, and if those are tolerated, water is given. The intravenous line remains in place until clear liquids can be taken and tolerated. This may occur almost immediately following surgery, especially if a local anesthetic was used. Sometimes general anesthesia can induce nausea, which may delay taking oral fluids. Once clear liquids are tolerated, the diet progresses to solid foods.
Patients are transferred from the PACU to the outpatient or ambulatory unit, where recovery is completed. Inpatients return to their room. Most patients go home once they are up and walking around. Even though the anesthesia has worn off, most patients remain groggy for the rest of the day. Patients must make arrangements for a family member or friend to be with them upon discharge if they are going home the day of surgery.
Spinal anesthesia usually wears off within a few hours. In the first hour following surgery, patients usually lie flat on their back to decrease the chance of an anesthetic-induced headache, which can be painful and prolonged. A patient must regain full sensation in the region of their body that was numbed before being discharged.
Patients experience pain at the incision site, especially conventional procedure patients. Medication is prescribed and taken as directed. Swelling and discoloration usually develops around the incision and eventually disappears in the healing process. Some soreness can be expected during the first 24 to 48 hours.
The tiny incisions made during laparoscopic surgery are held together by steri-strips that fall off in about a week to 10 days. Patients can take a shower within two days after surgery. Regular sutures or staples usually hold together the large incision made in the open procedure. The wound must be kept dry until it begins to heal, so patients may have to take sponge baths for the first few postoperative days to avoid getting the wound wet.
Prevention
You can’t prevent the congenital defect that makes you susceptible to an inguinal hernia. You can, however, reduce strain on your abdominal muscles and tissues. For example:
- Maintain a healthy weight. Talk to your doctor about the best exercise and diet plan for you.
- Emphasize high-fiber foods. Fruits, vegetables and whole grains contain fiber that can help prevent constipation and straining.
- Lift heavy objects carefully or avoid heavy lifting. If you must lift something heavy, always bend from your knees — not your waist.
- Stop smoking. Besides its role in many serious diseases, smoking often causes a chronic cough that can lead to or aggravate an inguinal hernia.
- Don’t rely on a truss. Wearing a supportive garment designed to keep hernias in place (hernia truss) doesn’t correct the problem or help prevent complications. Your doctor might recommend a hernia truss for a short time before surgery to help you feel more comfortable, but the truss isn’t a replacement for surgery.