


Definition
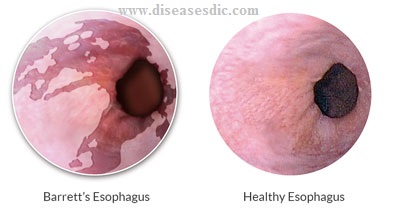
Barrett’s esophagus is a disorder in which the lining of the esophagus is damaged. This damage occurs when parts of the esophageal lining are repeatedly exposed to stomach acid, and are replaced by tissue that is similar to what is found in the intestine. Barrett’s esophagus can lead to Esophageal cancer if left untreated.


The esophagus is the feeding tube that delivers food and liquids to the stomach. The stomach produces acid to aid in digestion of the food and drink we consume. Barrett’s esophagus is a disorder in which the lining of the esophagus is damaged by long standing acid reflux. Barrett’s esophagus can lead to esophageal cancer if left untreated.

History
The condition is named after Australian thoracic surgeon Norman Barrett (1903–1979), who in 1950 argued that ′ulcers are found below the squamocolumnar junction represent gastric ulcers within “a pouch of stomach drawn up by scar tissue into the mediastinum” representing an example of a “congenital short esophagus”′.
In contrast, Philip Rowland Allison and Alan Johnstone argued that the condition related to the ″esophagus lined with gastric mucous membrane and not intra-thoracic stomach as Barrett mistakenly believed.″
Philip Allison, cardiothoracic surgeon and Chair of Surgery at the University of Oxford, suggested ″calling the chronic peptic ulcer crater of the esophagus a “Barrett’s ulcer″, but added this name did not imply agreement with ″Barrett’s description of an esophagus lined with gastric mucous membrane as stomach.
Types of Barrett’s esophagus
Non-dysplastic (NDBE)
NDBE has the salmon-pink coloring of intestinal type mucosa, but no worrisome cellular changes. Dysplasia progresses, or gets worse, over time when genetic changes in the tissue add up.
Low-grade dysplasia (LGD)
LGD has features of mildly atypical cells (larger cells with some distortion).
High-grade dysplasia (HGD)
HGD cells are larger and tend to appear more disorganized. Therefore, have many worrisome features that are considered much more likely to develop into cancer.
Risk factors
- Obesity (especially in men who store large amounts of belly fat)
- Smoking
- Consuming rich foods high in fat (which forces the stomach to produce lots of acid to break down the food)
- Possible genetic predisposition
- Over 50 years old
Barrett’s esophagus causes
Barrett’s Esophagus is caused by excessive exposure to stomach acid and is most commonly found in patients with ongoing GERD (gastroesophageal reflux disease). GERD is characterized by long-term regurgitation of stomach acid into the lower esophagus.
Symptoms
The following are the most common symptoms of Barrett’s esophagus. However, each individual may experience symptoms differently. Symptoms may include:
- Waking in the night because of heartburn pain
- Vomiting
- Difficulty in swallowing
- Blood in vomit or stool
Some persons with this condition may be asymptomatic. The symptoms of Barrett’s esophagus may resemble other medical conditions or problems.
Complications
- Barrett’s esophagus is a premalignant (precancerous) condition that may lead to the development of cancer of the esophagus in a small number of patients. The risk of developing cancer is approximately 0.3% each year. This type of cancer is called esophageal adenocarcinoma.
- Esophageal cancer develops through a sequence of changes, known as dysplasia, in the cells of the esophagus. Dysplasia can only be detected by endoscopic biopsies. Patients with Barrett’s esophagus should have regular surveillance exams to detect cancer at an early and potentially curable stage.
Diagnosis and test
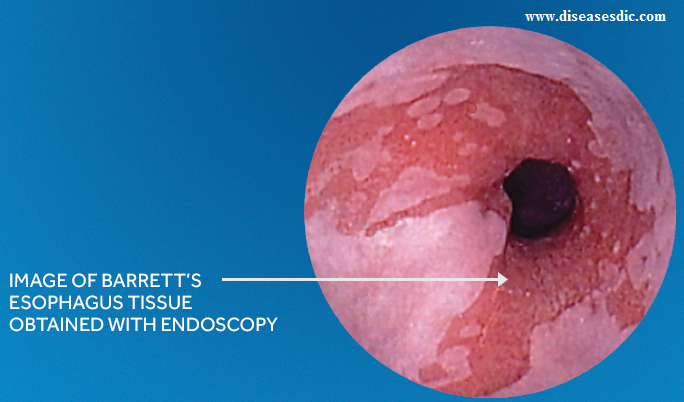
Doctors diagnose Barrett’s esophagus with an upper gastrointestinal (GI) endoscopy and a biopsy. Doctors may diagnose Barrett’s esophagus while performing tests to find the cause of a patient’s gastroesophageal reflux disease (GERD) symptoms.
Medical history
Your doctor will ask you to provide your medical history. Your doctor may recommend testing if you have multiple factors that increase your chances of developing Barrett’s esophagus.
Upper GI endoscopy
In an upper GI endoscopy, a gastroenterologist, surgeon, or other trained health care provider uses an endoscope to see inside your upper GI tract, most often while you receive light sedation. The doctor carefully feeds the endoscope down your esophagus and into your stomach and duodenum. The procedure may show changes in the lining of your esophagus.
Biopsy
The doctor performs a biopsy with the endoscope by taking a small piece of tissue from the lining of your esophagus. You won’t feel the biopsy. A pathologist examines the tissue in a lab to determine whether Barrett’s esophagus cells are present. A pathologist who has expertise in diagnosing Barrett’s esophagus may need to confirm the results.
Barrett’s esophagus can be difficult to diagnose because this condition does not affect all the tissue in your esophagus. The doctor takes biopsy samples from at least eight different areas of the lining of your esophagus.
Treatment of Barrett’s esophagus
Endoscopic surveillance
Every three years, the physician will used an endoscope to check the lining of the esophagus to see if any abnormal tissue is present, and can remove a small sample to examine (biopsy).

Dilation treatment
You may need this if you have a narrowing of the esophagus. During dilation, a tool gently stretches (dilates) the narrowed part of the esophagus. It also widens the opening of the esophagus.
Endoscopic radio frequency ablation therapy
This treatment destroys the pre-cancerous tissue in the lining of the esophagus that occurs with Barrett’s esophagus. During the procedure, an ablation catheter (HALO360 or HALO90 Ablation Catheter) is positioned on the abnormal esophageal tissue. Using the HALO Energy Generator, the physician delivers a rapid burst of ablative energy, which removes a very thin layer of the diseased esophagus by heating it.
Surgery
A type of surgery called fundoplication takes out damaged tissue or part of the esophagus. The part of the esophagus that is left is usually joined to the stomach.
Medications
If lifestyle and dietary changes do not work, medications may be prescribed. There are two categories of medicines for reflux. One decreases the level of acid in your stomach, and one increases the level of motility (movement) in the upper gastrointestinal tract.
Antacids
Over-the-counter antacids are best for intermittent and relatively infrequent symptoms of reflux. When taken frequently, antacids may worsen the problem. They leave the stomach quickly, and your stomach actually increases acid production as a result.
Histamine Blockers
Histamine 2 (H2) blockers are drugs that help lower acid secretion. H2 blockers heal esophageal erosions in about 50 percent of patients.
Proton Pump Inhibitors
Proton pump inhibitors (PPIs) are drugs that block the three major pathways for acid production. PPIs suppress acid production much more effectively than H2 blockers. PPIs are the most effective medication for healing erosive esophagitis and providing long-term control of GERD symptoms.
Prokinetic Agents
Prokinetic agents are drugs that enhance the activity of the smooth muscle of your gastrointestinal tract. These drugs are somewhat less effective than PPIs. These may be prescribed in combination with an acid-suppressing drug.
Lifestyle and home remedies
Lifestyle changes can ease symptoms of GERD, which may underlie Barrett’s esophagus. Consider:
- Maintaining a healthy weight.
- Eliminating foods and drinks that trigger your heartburn, such as chocolate, coffee, alcohol and mint.
- Stopping smoking.
- Raising the head of your bed. Place wooden blocks under your bed to elevate your head.
Prevention of Barrett’s esophagus
Since Barrett’s esophagus is usually the direct result of gastroesophageal reflux disease, controlling or curbing the effects of GERD can help prevent Barrett’s esophagus from developing.
Researchers have not found that diet and nutrition play an important role in causing or preventing Barrett’s esophagus.
If you have gastroesophageal reflux (GER) or gastroesophageal reflux disease (GERD), you can prevent or relieve your symptoms by changing your diet. Dietary changes that can help reduce your symptoms include
- Decreasing fatty foods
- Eating small, frequent meals instead of three large meals
Avoid eating or drinking the following items that may make GER or GERD worse:
- Chocolate
- Coffee
- Peppermint
- Greasy or spicy foods
- Tomatoes and tomato products
- Alcoholic drinks